Expo
view channel
view channel
view channel
view channel
view channel
view channel
view channel
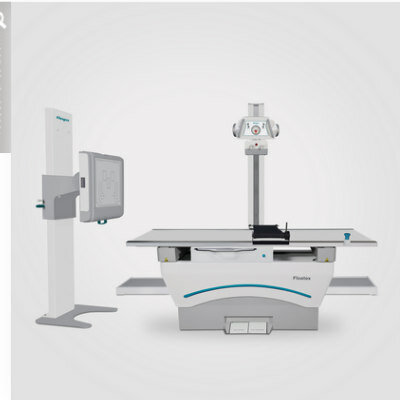
Medical Imaging
AICritical CareSurgical TechniquesPatient Care
Point of CareBusiness
Events
Webinars

- AI Analysis of EMS Calls Aids Pediatric Trauma Decision-Making
- Home Exercise Program Advances Recovery After Aortic Dissection
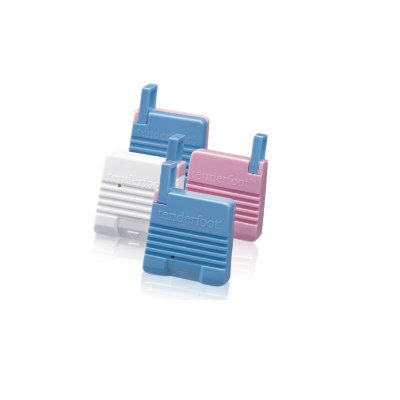
- Noninvasive Silk Sensor Could Transform Care for Premature Infants
- AI Identifies Hidden Stroke Risk Through At-Home Behavior Patterns
- AI-Guided Outreach System Improves Colorectal Cancer Screening
- Focused Ultrasound System Gains CE Mark for Liver Tumor Treatment
- New Near-Infrared Dye Enables Prolonged Ureter Visualization During Surgery
- FDA Clears Robotic System for Precise TMS Coil Positioning
- Novel Microparticles Break Down Biofilms and Boost Antibiotic Activity
- Nerve Block Technique Reduces Opioid Use After Cardiac Surgery
- Wearable Sleep Data Predict Adherence to Pulmonary Rehabilitation
- Revolutionary Automatic IV-Line Flushing Device to Enhance Infusion Care
- VR Training Tool Combats Contamination of Portable Medical Equipment
- Portable Biosensor Platform to Reduce Hospital-Acquired Infections
- First-Of-Its-Kind Portable Germicidal Light Technology Disinfects High-Touch Clinical Surfaces in Seconds
- Danaher Completes Acquisition of Masimo to Expand Patient Monitoring Capabilities
- Endologix Adds FDA-Cleared Peripheral Thrombectomy System
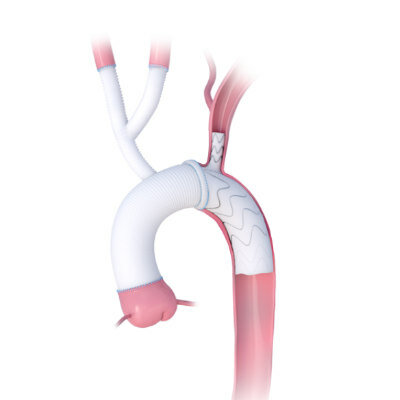
- Artivion Adds FDA-Approved NEXUS System to Aortic Arch Portfolio
- Olympus Partnership Aims to Expand Access to Robot-Assisted Endoscopic Therapy
- Johnson & Johnson Launches AI-Driven Cardiac Mapping System
- Digital Heart Model Supports Targeted Ablation in Atrial Fibrillation
- AI Framework Helps Clinicians Create Trustworthy Risk Prediction Tools
- AI Tool Screens for Primary Aldosteronism Using Routine EHR Data
- AI-Enabled ECG Software Predicts One-Year Atrial Fibrillation Risk
- AI-Native EHR Achieves EU Medical Device Certification
- AI Trends Report Guides Responsible, Effective Healthcare Deployment
- Privacy-Preserving AI Protects Sensitive Information in ECG Data
- New AI ECG Tool Detects Early Heart Disease
- AI Platform Supports Noninvasive Remote Hemodynamic Monitoring in Heart Failure
- AI Tool Predicts Unplanned Care and Symptom Burden in Cancer Survivors
- Handheld Ultrasound Expands Point-of-Care Imaging Access in Brazil
- AI Dermatology Platform Targets Early Detection of Non-Melanoma Skin Cancer
- Handheld AI Device for Point-of-Care Skin Lesion Assessment Receives CE Mark
- Portable Immunoassay System Advances Toward Point-of-Care Biomarker Testing
- Portable MRI System Accelerates Emergency Brain Imaging and Triage
- AI Analysis of EMS Calls Aids Pediatric Trauma Decision-Making
- Home Exercise Program Advances Recovery After Aortic Dissection
- Noninvasive Silk Sensor Could Transform Care for Premature Infants
- AI Identifies Hidden Stroke Risk Through At-Home Behavior Patterns
- AI-Guided Outreach System Improves Colorectal Cancer Screening
- Focused Ultrasound System Gains CE Mark for Liver Tumor Treatment
- New Near-Infrared Dye Enables Prolonged Ureter Visualization During Surgery
- FDA Clears Robotic System for Precise TMS Coil Positioning
- Novel Microparticles Break Down Biofilms and Boost Antibiotic Activity
- Nerve Block Technique Reduces Opioid Use After Cardiac Surgery
- Wearable Sleep Data Predict Adherence to Pulmonary Rehabilitation
- Revolutionary Automatic IV-Line Flushing Device to Enhance Infusion Care
- VR Training Tool Combats Contamination of Portable Medical Equipment
- Portable Biosensor Platform to Reduce Hospital-Acquired Infections
- First-Of-Its-Kind Portable Germicidal Light Technology Disinfects High-Touch Clinical Surfaces in Seconds
- Danaher Completes Acquisition of Masimo to Expand Patient Monitoring Capabilities
- Endologix Adds FDA-Cleared Peripheral Thrombectomy System
- Artivion Adds FDA-Approved NEXUS System to Aortic Arch Portfolio
- Olympus Partnership Aims to Expand Access to Robot-Assisted Endoscopic Therapy
- Johnson & Johnson Launches AI-Driven Cardiac Mapping System
- Digital Heart Model Supports Targeted Ablation in Atrial Fibrillation
- AI Framework Helps Clinicians Create Trustworthy Risk Prediction Tools
- AI Tool Screens for Primary Aldosteronism Using Routine EHR Data
- AI-Enabled ECG Software Predicts One-Year Atrial Fibrillation Risk
- AI-Native EHR Achieves EU Medical Device Certification
- AI Trends Report Guides Responsible, Effective Healthcare Deployment
- Privacy-Preserving AI Protects Sensitive Information in ECG Data
- New AI ECG Tool Detects Early Heart Disease
- AI Platform Supports Noninvasive Remote Hemodynamic Monitoring in Heart Failure
- AI Tool Predicts Unplanned Care and Symptom Burden in Cancer Survivors
- Handheld Ultrasound Expands Point-of-Care Imaging Access in Brazil
- AI Dermatology Platform Targets Early Detection of Non-Melanoma Skin Cancer
- Handheld AI Device for Point-of-Care Skin Lesion Assessment Receives CE Mark
- Portable Immunoassay System Advances Toward Point-of-Care Biomarker Testing
- Portable MRI System Accelerates Emergency Brain Imaging and Triage




")
")
 Model development using VAE with adversarial training to remove demographic attributes from ECGs. (B) Performance analysis for downstream tasks. (C) Applications of the privacy-preserving ECG embeddings in clinical outcome prediction and secure data sharing. (Fairuz Shadmani Shishir et al., Scientific Reports (2026). DOI: 10.1038/s41598-026-47665-6)")
")
")


")
")
")
. DOI: 10.1038/s41566-026-01945-9")

")
")
")
")
. (Photo courtesy of Longeviti Neuro Solutions)")
")
")
")
")



